Audiology
Vol. 44: Issue 6 - December 2024
Effects of face protector devices on acoustic parameters of voice
Abstract
Cover Image
Objectives. The SARS-CoV-2 pandemic required the use of personal protective equipment (PPE) in medical and social contexts to reduce exposure and prevent pathogen transmission. This study aims to analyse possible changes in voice and speech parameters with and without PPE.
Methods. Speech samples using different types of PPE were obtained. Recordings were then analysed using PRAAT software (version 6.1.42). Statistical analysis was conducted using ANOVA in Jamovi software. A post-hoc test was performed to compare PPE-related results.
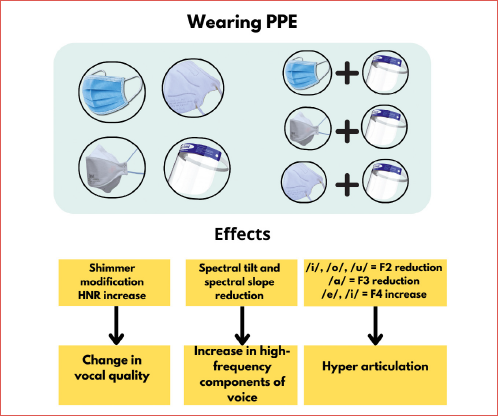
Results. Statistically significant differences were found in Cepstral Peak of Prominence- Smoothed, Harmonic to Noise Ratio (HNR), slope of Long-Term Average Spectrum (LTAS), tilt of trendline through LTAS, shimmer parameters, HNR mean and standard deviation of vowels, vowels and consonants formants. HNR values increased whereas shimmer parameters and formant values reduced using PPE [PPE combined>filtering face piece (FFP)> surgical masks>no PPE].
Conclusions. Our data show improvement in many parameters of voice and speech quality and modification of speech articulation when using masks, particularly in case of combined PPE. The most relevant changes were found with a combination of face shield and FFP2 masks. This may be due to unconscious improvements in speech articulation and increased demand on vocal folds to achieve better speech intelligibility.
Introduction
The use of personal protective equipment (PPE) is essential in preventing exposure to and transmission of pathogens in hospital and indoor settings 1. The selection of surgical masks, face-filtering respirators or face shields must ensure effective filtration capacity and fit.
Nevertheless, the use of PPE affects sound intensity and direction. For example, face shields deflect sound laterally or backward 2. PPE negatively affects voice quality and speech intelligibility 3,4. Several studies 5-8 suggest that facial masks act as low-pass filters, attenuating high frequencies (2-7 kHz). Surgical masks reduce sound intensity by 3-4 dB, whereas filtering face piece (FFP) masks by about 12 dB 7. PPE also attenuates frequencies between 1 and 8 kHz, with surgical masks attenuating by 2 dB and FFP masks attenuating by 5.2 dB. Additionally, the use of facemasks increases the LH1000 (low frequency energy/high frequency energy) ratio by an average of 2.5 dB for surgical masks and 5.2 dB for FFP masks 7. PPE limits sound projection and restricts articulatory movement 8. It produces an average increase in vocal intensity by about 2 dB and causes vocal fatigue, resulting in discomfort in the vocal tract 4. Finally, PPE significantly affects hearing aid and cochlear implant users, limiting their ability to lip-read 9.
This study aims to analyse the impact of four different PPE (surgical masks, FFP2 fold-flat facial filters, FFP2 3M™ Aura™ 9320+ facial filters, face shield) and combinations of them (face shield combined with: i) surgical mask; or ii) with FFP2 fold flat; iii) with FFP2 3M™ Aura™ 9320+) on various acoustic parameters, namely fundamental frequency, Jitter Local (JL), Shimmer Local (SL), shimmer dB, Harmonic to Noise Ratio (HNR), Acoustic Voice Quality Index (AVQI), Cepstral Peak of Prominence-Smoothed (CPPS), spectral tilt and spectral slope. Secondly, this study aims to evaluate how these changes impact articulation skills by analysing the changes in formant transitions.
Materials and methods
Participants meeting the following inclusion criteria were recruited for this study in July and August 2021: age of 18 years and above with no personal history of hearing impairment or vocal diseases as stated by the participants. Participants who were not able to sustain an /a/ sound for at least 3.5 seconds were excluded. Following those criteria, 20 Italian participants (4 males, 16 females) aged between 21 and 61 [mean ± standard deviation (SD): 32.9 ± 13.7 years] were included in the study following informed consent. All provided negative COVID test results as part of their recruitment. Speakers were recorded using LingWAVES 2.6 software, a WEVOSYS microphone, and a LingWAVES SPL meter II (IEC 651, ANSI S1.4 Type 2) on a Windows 7 operating system. The files were acquired in MONO format, with a resolution of 16 bits and a sampling frequency of 44.1 kHz. No gain adapters, peak limiters or compressors were employed. Voice samples were recorded inside a soundproof booth with a background noise level below 30 dB.
Microphone height was adjusted to match the participant’s floor-to-mouth height. The microphone stand was positioned 30 cm away from the speaker’s mouth. Every 10 minutes, speakers were asked to take a sip of water and have a break. An individual audio file was recorded both without any PPE and with each type of device (surgical mask, FFP2 fold-flat facial filter, FFP2 facial filter 3M™ Aura™ 9320+, face shield, face shield combined with surgical mask, face shield combined with FFP2 fold flat, face shield combined with FFP2 3M™ Aura™ 9320+), in a random order. Most subjects started the recording without PPE or using the one they were already wearing. They were instructed to stand directly in front of the microphone in a natural position and were given no specific instructions on how to speak, except to produce a natural sound emission.
The recording protocol consisted of (a) sustained vowel sounds (/a/, /e/, /i/, /o/, /u/) for at least 2.5 seconds, (b) 10 syllables (/a/+C+/a/) with Italian voiced or voiceless stop or fricative consonants: /p/, /b/, /t/, /d/, /k/, /g/, /z/, /f/, /v/, /ʃ/, and (c) sentences taken from Consensus Auditory-Perception Evaluation of Voice (CAPE-V) 10, specifically the first two of five phonetically balanced sentences in the Italian language.
For each participant, 16 different vocal samples (5 vowels + 10 syllables + 1 sample with sentences) were recorded and a total of 2560 files (20 subjects x 8 recording device x 16 speech portions) were analysed.
For sustained vowels, several parameters were detected, including JL, SL, HNR 3. The same samples were used to analyse values of jitter rap, jitter ppq5, jitter ddp, shimmer dB, shimmer apq3, shimmer apq5, shimmer apq11, and shimmer dda in order to define the specific features of jitter and shimmer parameters. PRAAT software (version 6.1.42) was used to extract acoustic spectrum parameters CPPS, HNR, slope of Long-Term Average Spectrum (LTAS) and tilt of trendline through LTAS from the initial audio files of the vowels. To obtain an objective evaluation of voice quality, the AVQI was measured by analysing both sustained vowels and continuous speech. Furthermore, 10 syllables (consisting of the vowel /a/ and occlusive or fricative consonants such as /p/, /b/, /t/, /d/, /k/, /g/, /z/, /f/, /v/, /ʃ/ followed by the vowel /a/) were considered to detect formants. The data were manually segmented using TextGrid-PRAAT software.
The statistical software Jamovi (version 1.8) was utilised for statistical analysis. A two-way analysis of variance (ANOVA) was conducted to examine the impact of the independent variable device on the dependent variables represented by the individual parameters. For the parameters that exhibited statistical significance (p < 0.05), a post-hoc test was carried out using a many-to-one comparison approach, comparing the results obtained with all devices. Statistical significance was set at p < 0.05.
Results
The ANOVA indicated significant differences in CPPS, HNR, slope of LTAS, and iilt of trendline through LTAS (Fig. 1). Significance was found even for shimmer parameters, HNR mean, SD of vowels and for vowels and consonant formants (Figs. 2-3). Post-hoc test analyses (Tabs. I-IV) were conducted to compare the condition without PPE to every different PPE condition.
No PPE – surgical mask
Results show that wearing surgical masks reduces SL by 0.067%, shimmer dB by 0.06 dB, shimmer apq3 and apq5 by 0.004 dB, and shimmer dda by 0.012 dB for the vowel /e/. The HNR for the vowels /e/ and /i/ increased by 2.3 dB and 2 dB, respectively. Additionally, the first formant of the vowel /a/ decreased by an average of 3 Hz, while the second formant increased by 3 Hz. The third formant of the vowel /e/ showed an average decrease of 152 Hz. Similarly, the third and fourth formants of the vowel /i/ were reduced by an average of 234 Hz and 258 Hz, respectively. As for the acoustic spectral parameters, surgical masks resulted in an average decrease of 0.8 dB in the spectral tilt (tilt of trendline through LTAS).
No PPE – FFP2 3M™Aura™ 9320+ mask
The FFP2 3M™ Aura™ 9320+ mask had an impact on several important parameters. SL and shimmer dB of the vowel /e/ were reduced on average by 1.13% and 0.101 dB. Similar trends were observed for shimmer apq3, shimmer apq5, shimmer apq11, and shimmer dda. The SL and shimmer dB of vowel /i/ also showed a decrease of 0.71% and 0.06 dB, respectively. The HNR values for the sustained vowels /e/ and /i/ significantly increased by 3.9 dB and 4.1 dB respectively. Spectral tilt only was reduced by an average of 0.8 dB in spectral parameters.
The usage of the FFP2 3M™ Aura™ 9320+ mask resulted in a decrease in the values of formants F1, F2, and F3 for the vowel /a/ (decreased by 31 Hz, 1 Hz, and 279 Hz respectively) and all minimum and maximum values of the three formants. The values of F2 and F3 for the vowels /e/ and /i/ were reduced by 205 Hz and 238 Hz, respectively, for /e/, and by 195 Hz and 188 Hz, respectively, for /i/.
No PPE - FFP2 fold-flat mask
The FFP2 fold-flat mask increased the HNR value by 1.3 dB in the LTAS and by 3.8 dB and 3.4 dB in sustained vowels /e/ and /i/ respectively. The shimmer parameters for vowels /e/ and /i/ were reduced. The spectral slope and spectral tilt decreased significantly by 2.81 dB and 1.2 dB respectively. The F3 of vowel /a/, F2, F3, and F4 of vowels /e/ and /i/ were lower, measuring 227 Hz, 198 Hz, 249 Hz, and 370 Hz, respectively. An increase in the frequencies of F2, F3, and F4 of vowel /i/ was detected, measuring 290 Hz, 230 Hz, and 201 Hz, respectively, along with an increase in the average values of the maximum and minimum for each of these formants.
No PPE - face shields
Face shields decreased the SL and shimmer dB values of the vowels /e/ and /i/ by 1.23% (0.108 dB) and 0.95% (0.084 dB) respectively. The HNR showed an average increase of 2.2 dB in the LTAS and increases of 5.9 dB for vowel /e/, 6 dB for vowel /i/, and 2.6 dB for vowel /o/. The SD of HNR increased by 0.64 dB in the vowel /u/. Additionally, face shields reduced the values of CPPS, spectral slope, and spectral tilt by an average of 1.6, 8.41 dB, and 0.9 dB, respectively. The F1, F2, and F3 formants of the vowel /a/ were decreased by 111 Hz, 103 Hz, and 245 Hz, respectively, while F2 of vowel /e/ decreased by 199 Hz. The F4 formant of vowel /e/ increased by 192 Hz, and F2 of vowels /i/, /o/, and /u/ decreased by 265 Hz, 94 Hz, and 83 Hz, respectively. Furthermore, the initial frequency of the formant transition of consonant /p/ and the final frequencies of formant transitions of /t/ and /k/ showed a decrease.
No PPE – face shield + surgical mask
The combination of a face shield and a surgical mask increased the HNR values of vowels /e/, /i/, and /u/. The SL parameters changed in vowels /e/ and /i/, with a decrease of 0.89% and 0.75%, respectively. The shimmer dB value was reduced on average by 0.076 dB in vowel /e/ and by 0.065 dB in vowel /i/. The amplitude perturbation parameters CPPS, spectral slope, and spectral tilt were also decreased by an average of 1.6, 8.41 dB, and 1.5 dB, respectively. The F1, F2, and F3 pitches of vowel /a/ were lower (by 110 Hz, 114 Hz, and 326 Hz respectively), as were F2 and F3 of vowel /e/ (by 243 Hz and 164 Hz, respectively) and F2 of vowel /i/ (by 328 Hz). The formant transition of /p/ was decreased on average by 97 Hz, while the transitions of /v/, /k/, and /ʃ/ were decreased by 79 Hz, 123 Hz, and 138 Hz, respectively.
No PPE – face shield + FFP2 3M™ Aura™ 9320+ mask
The combination of the face shield and FFP2 ‘platypus’ modified the shimmer and HNR parameters. The mean and SD of HNR increased by 8.3 dB and 0.7 dB in the vowel /e/, by 8 dB in the vowel /i/, and by 0.89 dB in the vowel /u/. The spectral CPPS value decreased by 1, the spectral slope value decreased by 8.41 dB, and the spectral tilt value decreased by 1.4 dB. The F1 and F3 formants of the vowel /a/, and the F2 and F3 formants of the vowel /e/ and /i/ decreased. In addition, the transitions of /d/, /z/, /g/, /ʃ/ amounted to 143 Hz, 110 Hz, 122 Hz, and 93 Hz, respectively.
No PPE – face shield + FFP2 fold-flat mask
The combination of a face shield and an FFP2 “parrot” mask resulted in a reduction in shimmer parameters for the vowel sounds /e/ and /i/. However, there was an increase in SL and shimmer dB for the vowel sound /u/. The mean and SD values of HNR increased by 7 dB and 0.87 dB, respectively, for the vowel /e/. Average HNR also increased for the vowel sounds /i/ and /u/. The formants F1, F2, F3 of the vowel sound /a/ were reduced by 123 Hz, 95 Hz, and 389 Hz, respectively. The same trend was observed for the F2 and F3 formants of the vowel sound /e/ (reduced by 347 Hz and 220 Hz, respectively), as well as for the F2 and F3 formants of the vowel sound /i/ (reduced by 465 Hz and 192 Hz, respectively), and the F2 formant of the vowel sound /u/ (reduced by 94 Hz). In addition, the final frequencies of the transitions /d/, /t/, /z/, /g/, and /k/ were decreased by 137 Hz, 118 Hz, 106 Hz, 182 Hz, and 146 Hz, respectively.
Our data suggest that using various devices leads to an increase in HNR in LTAS and the vowel sounds /e/ and /i/, as well as a decrease in Shimmer values, spectral tilt, and spectral slope. Many modifications in formants and transitions were observed with different PPE.
Discussion
Our study revealed changes in several acoustical voice parameters when using PPE, suggesting an improvement in vocal quality in limited phonation tasks due to an increase in the intensity of harmonics. We observed a gradual increase in HNR value, an important parameter for assessing vocal quality, in LTAS and for the vowels /e/ and /i/. Our results find support in the current literature, where an increase in HNR has been reported with surgical and KN95 masks 11.
Shimmer parameters were reduced when using different devices compared to the condition without PPE. Conversely, shimmer increased when wearing PPE in combination. In particular, the highest increase was noted using a face shield and surgical mask together. This suggests that performing voice assessment with a medical mask alters most of the acoustic and aerodynamic parameters. This result confirms what has been assessed in previous studies, where a reduction of jitter (%) and shimmer (%) values was found when the volume was increased, especially wearing a N95 mask .
In contrast to a previous report 3, these findings suggest that vocal quality improves due to an increase in the intensity of harmonics compared to noise in the voice. This discrepancy may be attributed to the different methods used to acquire vocal samples. Previous studies utilised dummies to produce sounds using devices 3,7. This condition leads to a difficult detection of the unconscious individual changes made by subjects during examinations 13. As facial PPE alters the configuration of articulatory organs and the intensity of emitted sound 14,15, we hypothesise that the subsequent involuntary hyper-articulation enriches the spectrum of vocal emission with harmonics. The SD of HNR results imply an increase in the variability of the values obtained.
The use of FFP2 masks, combined with a face shield, reduces the F3 frequency for the /a/ vowel, leading to increased protrusion of lips and slight retraction of the constriction in the oral cavity 16. As the oral constriction moves forward toward the palatal zone, F4 values for /e/ and /i/ vowels F4 increase 16. This may be due to the heightened intensity of speech and changes in articulation caused by the altered perception of one’s own voice. The emission of vowel /i/ using PPE, except for a face shield, leads to a decrease in F2. This aligns with the retraction of the oral constriction 16 due to the modified perception of words and limitations in movement while wearing PPE. Interestingly, the presence of a face shield and its combinations significantly decreases F2 for the posterior vowels /o/ and /u/, which is consistent with findings by Joshi et al. 17. This indicates hyper-articulation with lip protrusion 16, which is unconsciously performed in response to perceived resonance phenomena. In addition, Lin et al. found decrease in F3 and documented an increasing trend of F0, MPT, F1 and F2. Moreover, in that study, the change in loudness was much more evident than that in pitch due to the fact that participants tried to make their voices sound clearer wearing PPE 18.
Qualitative observation of formant transitions suggests that the use of a face shield and PPE leads to less linear formants, making it difficult to identify and manually segment them in the PRAAT software TextGrid.
To our knowledge, this is the first study on voice parameter modification with PPE analysing formants’ transition in syllables and spectral tilt. Spectral tilt, in particular, is increasingly relevant in the analysis of acoustic spectrum and vocal quality. The decreasing values of spectral tilt and spectral slope identified in the study, particularly noticeable with the use of face shields and their combinations with other devices, indicate an increase in the high-frequency component of the voice. This outcome directly suggests that delivering speech with these different devices requires greater vocal intensity: higher vocal intensity implies greater vocal effort and an emphasis on high frequencies rather than low frequencies in speech. Apparently, this is in contrast with some studies that found reduction of vocal intensity with PPE 3,7, and thus the condition may depend on sound emission with dummies, since there is no subjective and unconscious modification in sound emission. However, further study on vocal intensity is necessary to better define intensity modification in vocal emission with face devices. A qualitative analysis of the AVQI results also reveals that using face shields alone leads to an increase in AVQI values: the reflection and resonance waves caused by the face shield may negatively impact vocal quality.
Patients in the study reported greater difficulties when asked to speak with a face shield and FFP2 masks. The subjective increment in vocal effort during sound emission with PPE has been previously reported in literature and shown to cause difficulties in voice-breathing coordination 11: we qualitatively observed a reduction in phonation time and an increase in pauses during speech for air supply. During sustained speech, patients needed to adjust their airflow management by increasing the volume of inhaled air before phonation. This resulted in more vocal effort to compensate for the loss of energy. However, if this state persists, it can lead to dryness of the mucous membranes and dysfunctional behaviour, possibly causing organic and/or functional dysphonia 15. Future research should be dedicated to this topic.
Conclusions
This study demonstrated that PPE can alter various parameters of vocal tract articulation, voice quality, and speech formant values, especially when different types of PPE are used together. The reduction of shimmer and the improvement in HNR values with different devices demonstrates modification in voice quality related to the hyper-articulation of the vocal tract. These changes, although unconsciously perceived, lead to better speech emission during limited phonation tasks. These findings are supported by the reduction in negative spectral tilt and spectral slope values. CPPS values suggest that the use of a face shield negatively affects the harmonisation of the sound’s acoustic spectrum compared to the other PPE. In this regard, shimmer parameters and HNR values change the most when using surgical or FFP2 masks in combination with a face shield. However, it is important to note that the improvements in HNR and sound stability may be limited to recorded samples, while the effect of prolonged phonation with PPE is still not fully elucidated: prolonged speech may lead to increased vocal effort, which can result in worse vocal quality and increased vocal fatigue 15. Therefore, using only a surgical mask can limit changes in acoustic spectrum parameters and ensure better vocal quality with less fatigue. The necessity of increased vocal effort requires practice of good vocal hygiene and correct use of different speech modalities. Speech professionals should be consulted to provide proper guidance and explanations on the correct use of vocal modalities.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
VC, EZ, AM, EG, LM: conceptualisation; VC, EZ, AM, LM: methodology; VC, EZ, AM, LM: formal analysis and investigation; VC, EZ: writing - original draft preparation; VC, EZ, AM, RN: writing - review and editing; AM, EG: supervision.
Ethical consideration
This study was approved by the Institutional Ethics Committee of Emilia Nord Health District (protocol number 177/2020, March 11th, 2020) and by the Institutional Ethics Committee of University Hospital, Direzione Sanitaria dell’Azienda Ospedaliero-Universitaria, Modena (protocol number 7531, March 11th, 2020).
The research was conducted ethically with all study procedures being performed in accordance with the requirements of the World Medical Association’s Declaration of Helsinki. Written informed consent was obtained from each participant for study participation and data publication.
History
Received: December 5, 2023
Accepted: July 2, 2024
Figures and tables
Figure 1. Statistically significant spectral parameters of CPPS (A), HNR (B), slope of LTAS (C), and tilt (D).
Figure 2. Statistically significant parameters of vowel formants: /a/ formants (A), /e/ formants (B), /i/ formants (C), /o/ F2 formants (D), /u/ F2 formants (E).
Figure 3. Statistically significant values of vowel spectral parameters: /e/ shimmer local (A), /e/ shimmer dB (B), /i/ shimmer local (C), /i/ shimmer dB (D), /u/ shimmer local (E), /u/ shimmer dB (F).
Table I. a. Statistically significant parameters and their variations between no PPE and surgical mask and no PPE and FFP2 3M™ Aura™ 9320+.
Table I. b. Statistically significant parameters and their variations between no PPE and surgical mask and no PPE and FFP2 3M™ Aura™ 9320+.
Table II. a. Statistically significant parameters and their variations between No PPE and FFP2 fold-flat.
Table II. b. Statistically significant parameters and their variations between No PPE and FFP2 fold-flat.
Table III. a. Statistically significant parameters and their variations between no PPE – face shield and no PPE – shiel+FFP2 fold-flat.
Table III. b. Statistically significant parameters and their variations between no PPE – face shield and no PPE – shiel+FFP2 fold-flat.
Table IV. a. Statistically significant parameters and their variations between no PPE – shield+surgical mask and no PPE – shield+3M™ Aura™ 9320+.
Table IV. b. Statistically significant parameters and their variations between no PPE – shield+surgical mask and no PPE – shield+3M™ Aura™ 9320+.
References
- Infection Prevention and Control of Epidemic- and Pandemic-Prone Acute Respiratory Infections in Health Care. World Health Organization; 2014.
- Corey R, Jones U, Singer A. Acoustic effects of medical, cloth, and transparent face masks on speech signals. J Acoust Soc Am. 2020;148. doi:https://doi.org/10.1121/10.0002279
- Maryn Y, Wuyts F, Zarowski A. Are acoustic markers of voice and speech signals affected by nose-and-mouth-covering respiratory protective masks?. J Voice. 2023;37:468.E1-468.E12. doi:https://doi.org/10.1016/j.jvoice.2021.01.013
- Johnson A. Respirator masks protect health but impact performance: a review. J Biol Eng. 2016;10. doi:https://doi.org/10.1186/s13036-016-0025-4
- Mendel L, Gardino J, Atcherson S. Speech understanding using surgical masks: a problem in health care?. J Am Acad Audiol. 2008;19:686-695. doi:https://doi.org/10.3766/jaaa.19.9.4
- Nguyen D, McCabe P, Thomas D. Acoustic voice characteristics with and without wearing a facemask. Sci Rep. 2021;11. doi:https://doi.org/10.1038/s41598-021-85130-8
- Atcherson S, Mendel L, Baltimore W. The effect of conventional and transparent surgical masks on speech understanding in individuals with and without hearing loss. J Am Acad Audiol. 2017;28:58-67. doi:https://doi.org/10.3766/jaaa.15151
- Shindler A, Ginocchio D, Ricci Maccarini A. CAPE-V (Consensus Auditory-Perceptual Evaluation of Voice): Italian version. Acta Phoniatr Lat. 2006;28:383-391.
- Gama R, Castro M, van Lith-Bijl J. Does the wearing of masks change voice and speech parameters?. Eur Arch Otorhinolaryngol. 2022;279:1701-1708. doi:https://doi.org/10.1007/s00405-021-07086-9
- Yu M, Jin Q, Zhang W. Effects of different medical masks on acoustic and aerodynamic voice assessment during the COVID-19 pandemic. Medicine (Baltimore). 2023;102. doi:https://doi.org/10.1097/MD.0000000000034470
- Barsties V, Latoszek B, Jansen V. The impact of protective face coverings on acoustic markers in voice: a systematic review and meta-analysis. J Clin Med. 2023;12. doi:https://doi.org/10.3390/jcm12185922
- Muzzi E, Chermaz C, Castro V. Short report on the effects of SARS-CoV-2 face protective equipment on verbal communication. Eur Arch Otorhinolaryngol. 2021;278:3565-3570. doi:https://doi.org/10.1007/s00405-020-06535-1
- Ribeiro V, Dassie-Leite A, Pereira E. Effect of wearing a face mask on vocal self-perception during a pandemic. J Voice. 2022;36:878.e1-878.e7. doi:https://doi.org/10.1016/j.jvoice.2020.09.006
- Harrington J. The Handbook of Phonetic Sciences. (Hardcastle W, Laver J, Gibbon F, eds.). Blackwell Publishing Ltd.; 2010.
- Joshi A, Procter T. COVID-19: acoustic measures of voice in individuals wearing different facemasks. J Voice. 2021;37:971.e1-971.e8. doi:https://doi.org/10.1016/j.jvoice.2021.06.015
- Lin Y, Cheng L, Wang Q. Effects of medical masks on voice assessment during the COVID-19 pandemic. J Voice. 2023;37:802.e25-802.e29. doi:https://doi.org/10.1016/j.jvoice.2021.04.028
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2024 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 1059 times
- PDF downloaded - 267 times