Reviews
Vol. 44: Issue 6 - December 2024
A critical update on endoscopic dacryocystorhinostomy
Abstract
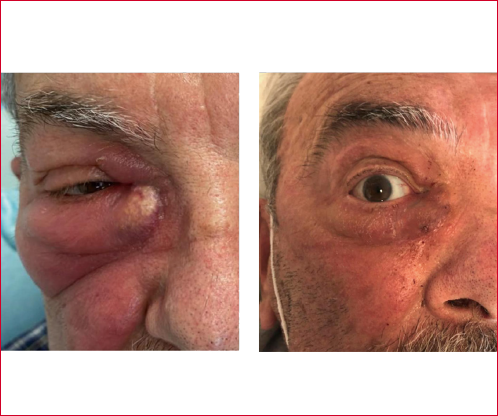
Cover Image
Objective. Endoscopic dacryocystorhinostomy (endo-DCR) is becoming a workhorse in the management of distal lacrimal duct obstruction. It yields success rates comparable to external DCR, with the advantage of no external scars. However, it requires multidisciplinary expertise and many uncertainties in terms of proper indications, technique, and perioperative management still exist.
Methods. Systematic review of the literature in the last 5 years using PubMed and Google Scholar.
Results. A total of 66 articles were included. Many technical modifications and surgical refinements have been proposed, but a formal comparison of the various techniques is hampered by methodological heterogeneity. The use of local anaesthesia and perioperative adjunctive techniques to reduce the risk of restenosis are also gaining popularity even if the level of evidence remains weak.
Conclusions. Endo-DCR offers satisfactory clinical outcomes even though there are many grey areas that need to be addressed in future high-quality studies.
Introduction
Dacryocystorhinostomy (DCR), whether performed by transnasal endoscopy (endo-DCR) or by external approaches (ext-DCR), is the cornerstone in the treatment of distal lacrimal duct obstruction 1. Its clinical effectiveness has been confirmed by several meta-analyses for both primary and revision cases, and the long-term success rates range from 89% to 94%, irrespective of the surgical approach or technique chosen, or the adjunctive methods used 2-4. Endoscopic endonasal techniques have gained much popularity because of their non-invasiveness, favourable cosmetic results, and functional outcomes which are comparable to classic external trans-facial approaches. They are also able to address concomitant nasal pathology that may favour the obstruction, yet they require multidisciplinary expertise in both ophthalmology and rhinology/otorhinolaryngology 2. The myriad of technological advances from high-definition endoscopes to the use of powered instruments has increased the diffusion of endo-DCR techniques. The literature is flourishing in this field and the present review aims to critically discuss the published evidence in the last five years on the medical and surgical management of endo-DCR. Furthermore, the current limitations and perspectives will be also highlighted.
Materials and methods
The present paper has been prepared following the recommendations of the PRISMA statement, and a modified PRISMA flowchart is given in Figure 1 5. The figure was generated using the freeware and web-based Shiny application that is made available by the group of Haddaway et al 6. No institutional review board approval was deemed necessary for the present review because no patient data was used. The Medline PubMed and Google Scholar databases were used to write the review with the searching period from January, 1st 2018 to June, 1st 2023. The following bibliographic string was used: “dacryocystorhinostomy OR DCR”. All pertinent articles were included after careful reading of the titles and abstracts. Full texts of the included articles were then retrieved by two authors (LGL and ERDZ) and quantitative and qualitative data were summarised accordingly. Abstracts were initially sorted by the specific techniques (external versus endonasal) that were exclusively or predominantly used in each article. We then excluded all non-relevant (e.g., ext-DCR) or off-topic papers; studies other than original articles or reviews, case series/reports, or written in languages other than English-French-Italian; papers investigating paediatric patients with congenital nasolacrimal duct obstruction.
The search strategy retrieved a total of 5,917 articles and, after applying the selection criteria and checking through the reference lists of the relevant studies, a total of 66 full texts were analysed (Fig. 1). Quantitative and qualitative data regarding surgical outcomes were summarised and systematically reported in tables.
Results
Optimal setting, timing, and perioperative management of patients with endo-DCR
In-office sinus surgery procedures have seen a steep rise in their use in the last decade given the well-known advantages of using local anaesthesia (LA) including faster recovery and lower costs 7. Endo-DCR is no exception to this trend and its favourable outcomes are presented by three recent experiences 8-10. In the first report, 84.6% of 77 patients showed complete resolution of epiphora, and LA (i.e., skin and intranasal infiltration plus neurosurgical cottonoids soaked in 5% cocaine) was used along deep sedation (propofol + fentanyl + midazolam) 8. Another group of authors performed an analysis of periprocedural pain with a simple Visual Analogue Scale (VAS) in 106 cases. They reported moderate pain (VAS 5-6) in 20.6% and no or mild pain for the remaining of the group with LA only; instead, no pain (VAS 0-2) was reported by all 14 patients who had LA + sedation (in this series, with pethidine and fentanyl) 9. Thirdly, Zhao et al. recently randomised 90 endo-DCRs into two groups (LA with dexmedetomidine + dezocine as adjuvants, N = 45) and a general anaesthesia (GA) group: the former type of anaesthesia showed more stable haemodynamics and was associated with lower VAS immediately after awakening and at 1, 2, 6, and 12 h postoperatively. Additionally, LA and sedation showed a lower incidence of postoperative agitation, nausea, and vomiting compared to GA 10. Regarding procedural complications related to the use of LA, accidental ingestion of nasal packing gauze and a potential risk of fire, when intranasal diathermy is used close to oxygen-delivering prongs, have been reported 8. Provokingly, in a recent case report of an endo-DCR under GA, the rupture of an intracranial aneurysm was associated with submucosal local infiltration with tetracaine and adrenaline (1:20,000) 11. Summing this up, a meta-analysis in 2022 including over 3200 endo-DCRs performed with GA and/or LA demonstrated that, even when powered instruments were used, a significant difference in success rates was noted between LA + sedation (85.1%, CI 77.8-90.4%), and GA (90.8%, CI 88.8-92.4%): however, due to the low number of publications, no conclusive statements were made 12.
As of when to perform an endo-DCR procedure, sound new evidence supports upfront operation in case of acute abscess or dacryocystitis. A small (43 patients) prospective randomised controlled trial from Finland demonstrated that “acute” endo-DCR (within 1 week from diagnosis) demonstrated no significant differences compared to delayed operations, in terms of lacrimal symptoms, syringing test, dye test, or use of resources at 18 months. The acute group, however, needed fewer analgesics than the delayed endo-DCR group with a median of 3 versus 10.5 days (p = 0.03) 13. Another study compared “very early” endo-DCR (within 3 days from the diagnosis) versus delayed ext-DCR, in adjunct with the same systemic antibiotics. By randomising 41 eyes, Pakdel et al. reported comparable anatomic and functional results, complications, and overall success between the two groups, but with a shorter duration of local cellulitis in the “very early” group 14. Complications (mostly skin fistula) were more frequent in the late DCR group from a large series from China (176 patients) that demonstrated significantly superior long-term outcomes when “urgent endo-DCR” (< 48 hours) was chosen 15. Finally, another retrospective study of 123 patients from South Korea reinforced the superiority of an aggressive upfront approach: in a sub-analysis, the time to symptom resolution, length of hospital stay, and duration of antibiotics were significantly shorter for the endo-DCR within 3 days compared to those receiving the operation between 4 to 7 days after diagnosis 16. Simultaneous bilateral endo-DCR is seldom required, but in a recent analysis of 128 cases where 13 were bilateral (26 sides), no significant differences emerged in terms of success and with the obvious advantages of sparing a second surgery 17.
As for the adjunctive treatments after endo-DCR, results on the use of stents are conflicting with two recent reports showing that routine placement of a lacrimal stent did not improve outcomes in either long-standing obstructions nor in cases of acute dacryocystitis 18,19. From a review of the literature in 2021, the intraoperative use of mitomycin C seems useful only in revision ext-DCR, and more recently, a meta-analysis on 739 eyes showed that the intraoperative application of hyaluronic acid significantly increased the success rate of endo-DCR (odds ratio = 3.27, 95% CI 2.15-4.98) 20,21.
The usefulness of steroids in reducing the risk of restenosis after endo-DCR is a more complex issue because of the different routes of administration. For instance, Chen et al. presented their experience with the intranasal placement of a steroid-soaked absorbable gelatin sponge to be left in the operated cavity. This work was retrospective and not randomised, but it appeared that significant improvement with this method was obtained (242 patients, a 92.5% success rate in the 55 with the sponge versus 83.6% in the group without) 22. Since intranasal haemostasis is often required after this procedure, an interesting experience on 407 eyes from South Korea showed that triamcinolone-soaked nasal packing was significantly superior to standard hygroscopic foams in terms of 6-month functional success (95 vs 89.3%, p = 0.033), equivalent in terms of anatomical patency (96 vs 92.7%, p = 0.149), and associated with a lower incidence of granulations (10 vs 20.4%, p = 0.003) 23. If packing is not needed as in mucosal preserving techniques, some authors discourage its use since it remains unproven that packing is associated with lower rates of postoperative synechiae, granulomas, or bleeding complications (all non-significant in a recent retrospective study where bio-packs were used) 24. Intuitively, thorough and regular endoscopic debridement after 2 weeks demonstrated a trend for better functional success (84.1% in the group without subsequent debridement versus 97.7% in those with debridement, p = 0.058) 25. Finally, regarding adjunctive steroids, a small series was published where 23 patients were randomised to use intranasal triamcinolone spray for 3 months postoperatively versus a control group of 25 after endo-DCR with stents. The success rates were not significantly different and treatment adherence was not assessed, but the authors used the lacrimal symptom questionnaire and reported significantly better results with the use of steroids 26.
Regarding the use of prophylactic antibiotics, a retrospective multi-institutional series of 331 endo-DCR cases performed at Boston Universities found that their use may be beneficial only when patients had a recent (within two weeks of surgery) or active dacryocystitis; in all other scenarios, their data do not support the routine use of antibiotic prophylaxis 27. These findings were also partially confirmed by a series of 152 patients from New York City where a history of dacryocystitis did not constitute a risk factor for postoperative infection 28.
In conclusion, the most recent meta-analysis on post-surgical medical adjunctive treatments dates to 2020 and included 18 papers on 3,590 external or endoscopic procedures 29. Given the lack of adequate data, the authors were able to carry out a meta-analysis only on endo-DCR outcomes and found no significant evidence for the use of nasal steroids (p = 0.58), oral antibiotics (p = 0.45), or nasal decongestants (p = 0.27) 29. Of note, the heterogeneity of the doses used and methods of administering adjunctive treatments as well as the lack of a standardised system to assess outcomes are still present in the current literature.
What is the best technique to perform DCR?
Endoscopic DCR is an effective surgical procedure whatever method is chosen, as reported in the review in 2020 by Vinciguerra et al. who analysed the pooled mean success rate of mechanical and powered endo-DCR, and established that there are no differences in outcomes (p = 0.43). In addition, mucosal flap preservation did not provide superior results (p = 0.14) 4.
However, the quest for the optimal technique persists, with emphasis placed on mucosal flap preservation, correct endonasal identification of the duct, use of flaps, type of powered instrument used to create the rhinostomy, management of concurrent nasal pathology, and treatment for concurrent canalicular and distal obstruction of the lacrimal pathway.
Regarding the former aspect, a study of 71 eyes proposed a “middle uncinate process approach” as a safer and more effective method (it is unclear compared to which technique), with a reported symptomatic success rate of 97.2%. This approach resulted in reduced surgical duration, precise localisation of the lacrimal sac, minimal bleeding, and eliminated the need for dilation tube insertion 30. Another variation of “classic” endo-DCR, named “retrograde” endo-DCR, was described by Alicandri-Ciufelli and colleagues 31. This modified approach is meant to be a safe procedure, even in patients with challenging anatomical conditions, because it allows easier identification of the lowermost part of the nasolacrimal duct, specifically at the level of the anterior insertion of the inferior turbinate. In most cases, at this level only a very thin shell of bone is present, and the duct is then followed upward along its course until the surgeon is able to unequivocally drill along the lacrimal pathway 31. Similarly, the “endonasal endoscopic nasolacrimal duct dissection” involved the removal of the bony structure covering the nasolacrimal duct, until it is marsupialised with nasal mucosa. In fact, according to Chang et al, postoperative outcomes, specifically resolution of epiphora, were comparable to those achieved with conventional endo-DCR. Furthermore, no major complications were reported intra- or postoperatively, although the authors did not report the operative time for this extended dissection 32. Finally, others have focused on the preoperative radiological identification of the duct: Ciger et al. found that the maxillary line-lacrimal sac anterior border distance was positively associated with the decrease in the duration of surgery (p = 0.000, r = 0.840) and the nasolacrimal duct obstruction symptom score (NLDO-SS) obtained after surgery (p = 0.041, r = -0.276). However, the differences are negligible since the standard deviation of this distance is 1 mm 33.
In 2022, Wang et al. proposed a modified seamless endoscopic dacryocystorhinostomy: the regular “I”-shaped incision was replaced by a “C”-shaped incision near the lateral bone window, and a gelatin sponge was applied at the confluence of the lacrimal sac and nasal mucosa, without any suture 34. They performed this approach in 32 patients, which was associated with a significantly shortened operation time and reduced bleeding compared to the 22 patients who underwent routine endo-DCR (p < 0.05). After 6 months of follow-up, the efficacy rate was significantly higher in the modified group than in the routine group (96.9 vs 68.2%; p < 0.05) 34. Endoscopic suturing and knotting-dacryocystorhinostomy is another proposal where the lacrimal sac mucosa is sutured with the nasal mucosa by tying knots under endoscopic view, without the use of a stent or mitomycin C 35. According to the proposing authors, this technique yielded anatomical and functional results that were unchanged during the 2-year follow-up period without serious complications. The endoscopic evaluation found that all patients showed a patent ostium and normal healing of the flaps after 4 weeks. The Munk scores decreased significantly at 6 months postoperatively compared to preoperative scores (p < 0.001) 35.
Several articles have explored the issue of the type of flaps and the method of harvesting. The lobulated pedicled nasal mucosa flap technique without stenting had a 100% anatomical patency success rate and a 94% symptomatic cure rate (63/67 patients), and there were no instances of complications in the experience of the proponents 36. In another study, the modified double-flap technique showed a lower recurrence rate compared to the single-flap technique: in a cohort of 77 cases the double flap covering the exposed lacrimal bone reduces postoperative obstruction over the nasolacrimal duct and ostium (recurrence rate of 3.2% in the double-flap group compared to 23.9% in the single-flap group, p = 0.022) 37. In the latest proposal, a clubhead-shaped nasal mucoperiosteal flap was combined with a posteriorly hinged lacrimal flap to create a tension-free anastomosis with the surrounding mucoperiosteum, although this technically demanding technique was only used in 8 cases, all with satisfactory outcomes 38.
In the context of flap-preserving techniques, there has been debate in the literature concerning the use of fibrin glue. In this regard, a recently published retrospective study reported that the surgical success rate was significantly higher in the fibrin glue anastomosis group (95.5%) than in the non-fibrin glue group (84.8%; p = 0.041), whereas the complication rate was similar in both groups (p = 0.99) 39.
It has not been definitively established whether mucosal flap preservation techniques offer any advantages over non-preserving techniques 40-43. The surgical success rate was not significantly different between endo-DCR with and without mucosal flap preservation in a population of 107 patients (82.1% without flap vs 86.8% with flap, p = 0.478) 40. Moreover, the complication rates between the two procedures were comparable, indicating that there is no discernible advantage in incorporating flap preservation 40. Likewise, in another study, long-term results suggest that mucosal flap preservation does not seem to be required to achieve successful outcomes in endo-DCR 41. Indeed, powered endoscopic DCR without preservation of mucosal flaps achieved complete resolution of epiphora in 93.1% of primary procedures and 68.8% of revision procedures. During endoscopic evaluation, objective anatomic patency was confirmed in 98% 41. Conversely, in a prospective randomised controlled trial, the group of patients undergoing a double mucosal flaps technique showed more satisfactory outcomes in terms of success rate compared to the group without flap preservation (97.9% compared to 89.6%, p = 0.092). The mucosal healing rate was also reported to be superior (p = 0.025) 42. Adding further confusion, in the 2023 study of Vatansever et al. mucosa-sparing surgery with a modified inverted U flap offered a significantly higher functional success rate compared to endo-DCR without mucosal flap and with less granulation tissue (p = 0.02) 43.
In the cases of concomitant proximal and distal obstruction, the application of a Castroviejo double-ended lacrimal dilator to facilitate the classic Jones tube insertion was recently described by Woo et al. 44. After being inserted, the lacrimal dilator created a direct fistula from the conjunctiva to the nasal cavity through the bony ostium: the Pyrex tube is then inserted into the fistula with a guidewire and secured in place by suturing. The success rate of this procedure was 73.4% and no serious complications were reported 44. A complex yet innovative approach was described by Ushio et al. in 2021, called conjunctivoductivo-dacryocystorhinostomy. This procedure involves an anastomosis of the conjunctiva and nasolacrimal duct without leaving any facial scars or foreign bodies in semi-permanent detention. Since the tip of the severed nasolacrimal duct is withdrawn back into the conjunctiva and directly sutured to the incision, the procedure did not necessitate the placement of a Jones tube 45.
The question of the clinical significance of preexisting nasal septal deviations remains unanswered. In a recent study, a concomitant septoplasty yields surgical success and associated complications equivalent to those of endo-DCR alone (no difference in anatomical success and functional success, p = 0.76 and p = 0.18, respectively) 46. However, in a systematic review by Kim et al. in 2020, performing a concurrent septoplasty or the use of a mucosal-preserving technique (irrespectively of the flap design) was judged as emerging (levels of evidence B and C) options to increase the chance of success of endo-DCR 20.
As technology advances, novel instruments are being experimented also with endonasal endoscopic surgery. The effect of the modified flap suture anastomosis technique using a Sonopet ultrasonic bone aspirator was retrospectively compared to that using a diamond burr in patients with nasolacrimal duct obstruction 47. The rates of successful suturing during the operation and of a large diameter of the lacrimal ostium 3 months after the operation were significantly higher in cases where the Sonopet was used 47. A robot-assisted endoscope positioning system that allows for hands-free visualisation of the surgical field was proposed in 2020. This device features a mechatronic holding arm and is driven by a foot pedal that can be precisely controlled. The surgeon can maintain bimanual instrumentation, which allegedly facilitated the dissection, but the report remains very preliminary 48.
A minimally-invasive alternative procedure is transcanalicular microdrill dacryoplasty: this is a variation of the external laser DCR where, under GA, the use of a 0.38 mm microdrill was reported to yield an 84% success rate with a very low rate of complications (0.2% of heavy postoperative bleeding) and 57.5% of patients presented full resolution of symptoms 49. In addition, balloon dacryoplasty (BD) is another option and a recent systematic review by Poignet et al. evaluated its results with and without silicone tube insertion 50. BD seems to be significantly more successful for partial nasolacrimal duct obstruction (success rate of 73.2%), while it is not effective for complete obstruction, with a disappointing success rate of 36.6%. The main complication is the high recurrence rate 50. Lastly, the use of chitosan-based dressing after endo-DCR with balloon dilation was associated with improved subjective and anatomical outcomes, compared to bioresorbable polyurethane packing versus no packing (p = 0.049), and reduced the need for revision surgery 51.
In conclusion, despite the variety of modified approaches, flaps or alternative procedures to classic endo-DCR, a retrospective analysis performed by Kumar et al. revealed that there are no significant differences in success rates, recurrences, or complications of various techniques at 3 or 6 months of follow-up. Moreover, BD was the technique associated with the shortest surgical time 52.
Reasons for and management of failures after primary DCR
Despite all the aforementioned techniques, a failure rate of approximately 10% is still present after endo-DCR, but the surgical or clinical factors contributing to procedural failure are not well defined. In an interesting retrospective research, significant correlations emerged between surgical failure and the presence of diabetes mellitus (that was also related to granulations) and allergy to medications. More obviously, granulations or adhesions in the osteotomy site correlated with surgical failure (p < 0.001). No correlations emerged for factors such as post-traumatic stenosis, previous nasolacrimal surgery, or the use of a stent 53. In another retrospective review, a significant correlation was observed between the lack of clinical improvement and several factors, including age, systemic conditions (including diabetes mellitus), or coexisting ophthalmological diseases and the time since the onset of the obstruction. Additionally, intraoperative findings such as a thickened lacrimal mucosa and the absence of flow when the sac is marsupialised were predictors of poor outcomes 54. Using multivariate analysis, Cohen et al. conducted a study to assess the 5- and 10-year success rates of endo-DCR and its associated covariates. They found that rates decreased over time and that long-term failure at 5 and 10 years after surgery was associated with older age, smoking, postoperative epiphora, and male gender 55. Regarding radiological predictive factors, in another report patients were categorised into three groups based on the preoperative pneumatisation of their ethmoid sinuses, as determined on computed tomography with dacryocystography. Unfortunately, the success rates were the same in the different radiological categories at 12 months 56.
Several options are available to manage a failed endo-DCR; however, identifying the precise osteotomy site and ensuring lasting patency pose significant challenges even if outcomes for revision cases are comparable to primary cases 57. An office-based salvage revision for impending rhinostomy failure after endo-DCR, utilising a microdebrider, was found to be effective in a small study. Among the 27 eyes studied, the causes of impending rhinostomy failure included granuloma formation (17/27 eyes), cicatrisation (8/27 eyes), and synechiae formation (2/27 eyes). All cases showed improvement in epiphora at 6 months 58. An Italian group introduced trans-nasal balloon-assisted dacryoplasty as a minimally-invasive surgical approach for treating failed DCRs. The procedure demonstrated reliable and stable long-term outcomes with a 100% anatomic success rate and an 85.7% functional success rate in 14 patients. The absence of post-surgical complications, a high success rate, and a short average operative time of 18 minutes make this innovative procedure noteworthy 59. Finally, Mueller et al. proposed a new technique for revision endo-DCR using a superior pedicled mucosal flap that provides excellent exposure of the maxillary bone and the lacrimal sac. In 13 procedures they achieved a success rate of 100% without complications after a mean follow-up of 26.9 ± 10.3 months 60.
Extreme and rare endo-DCR settings
While conventional DCR is effective in most cases, some patients present with unique anatomical variations or atypical conditions that demand specialised approaches. In such exceptional scenarios, innovative solutions become necessary for successful outcomes. The published evidence in the last 5 years on the extreme and rare endo-DCR settings is reported in Table I.
Unusual complications of endo-DCR
While endo-DCR is a well-established and effective surgery for most patients, there are instances where unusual complications can arise. We delve into some of these uncommon and unexpected complications associated with endonasal DCR. Understanding these atypical issues is crucial to ensure the best possible outcomes.
The published evidence in the last 5 years on the unusual complications of endonasal DCR is reported in Table II.
Conclusions
Endo-DCR is an umbrella term for a myriad of endoscopic procedures aimed at curing distal nasolacrimal duct obstruction with the advantage of no external approaches. Thanks to the availability of high-definition endoscopy and to new powered instruments the success rates are satisfactory, yet a one-technique-fits-all does not exist. In order to favour optimisation of resources and maximise patient satisfaction, a multidisciplinary team is necessary in every hospital wherever endo-DCR is performed.
Conflict of interest statement
All authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
LGL, ERDZ: conceptualisation, writing original draft; NC: data collection, supervision; AT: supervision, editing; PL, CM: conceptualisation, supervision.
Ethical consideration
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. No IRB approval was necessary due to the retrospective nature of this work. Informed consent: Informed consent was obtained from all individual participants included in the study.
History
Received: January 17, 2024
Accepted: June 11, 2024
Figures and tables
Figure 1. Identification of studies via databases and registers.
| No. | Author | Year | Study design | Sample size | Setting | Management | Outcome |
|---|---|---|---|---|---|---|---|
| 1 | Hsu et al. 61 | 2022 | Case report | 1 | Patient with a history of Caldwell-Luc surgery who developed considerable postoperative changes, reported epiphora in the last 5 years | Endo-DCR was performed with the aid of nasal forceps and a 20-gauge vitreoretinal fiberoptic endoilluminator | Complete resolution of symptoms and no signs of recurrence after 6 months |
| 2 | Gupta et al. 62 | 2021 | Case report | 1 | Blepharophimosis-ptosis-epicanthus inversus syndrome with congenital nasolacrimal duct obstruction | Endo-DCR | Not known |
| 3 | Sagar et al. 63 | 2018 | A case report and review of 18 cases | A case report and review of 18 cases | Primary nasolacrimal sac tuberculosis in a 15-year-old girl who presented with bilateral epiphora | Endo-DCR and anti-tubercular therapy (ATT). Treatment of tubercular dacryocystitis is ATT with surgery reserved for cases who remain epiphoric after medical treatment | Right eye epiphora improved while the left eye showed partial block due to synechia. Synechia release was done and patency was established |
| 4 | Song et al. 64 | 2020 | Case report | 1 | Localised amyloidosis involving the nasolacrimal duct and lacrimal sac | Endo-DCR and resection of multiple masses | One-year follow-up found no recurrence |
| 5 | Nassif et al. 65 | 2022 | Case report | 1 | Sinonasal sarcoidosis with nasolacrimal duct obstruction and dacryocystitis | Endo-DCR | 4 months postoperative follow-up showed resolution of nasal and ophthalmic symptoms |
| 6 | Azhdam et al. 66 | 2021 | Case report | 1 | Angioleiomyoma of the nasolacrimal duct | Endoscopic excision of the lesion along with medial maxillectomy and dacryocystorhinostomy | Resolution of the epiphora |
| No. | Author | Year | Study design | Sample size | Setting/complications | Management |
|---|---|---|---|---|---|---|
| 1 | Zhang et al. 11 | 2023 | Case report | 1 | Intracerebral and subarachnoid haemorrhage secondary to the rupture of an undiagnosed intracranial aneurysm | Stop surgery, stabilisation and recovery |
| 2 | Lee et al. 67 | 2021 | Case report | 1 | Delayed (after 1 month) unilateral pneumocephalus | Antibiotic therapy |
| 3 | Galindo-Ferreiro et al. 68 | 2021 | Case report | 1 | Orbital fat necrosis | The patient was given oral antibiotics and steroids for 2 weeks without any significant clinical improvement. Hence, the steroids were withdrawn and after a week, excisional biopsy was performed through a lid crease incision |
| 4 | Cheong et al. 69 | 2019 | Case report | 1 | Meningoencephalitis | Intravenous antibiotic treatment |
| 5 | Gungel et al. 70 | 2019 | Case report | 1 | Contralateral vision loss due to Purtscher-like retinopathy | 50 mg/0.1 mL of intravitreal tissue plasminogen activator injection |
| 6 | Bladen et al. 71 | 2020 | Retrospective, non-comparative case series | 7 | Peri-orbital surgical emphysema | Wait and see |
| 7 | Bothra et al. 72 | 2020 | Case report | 1 | Gossypibioma (retained surgical nasal pack) | Removal under endoscopic guidance followed by triamcinolone acetate injection into the base of the residual granuloma |
| 8 | Lee et al. 73 | 2020 | Case report | 1 | Optic neuropathy following DCR in a patient with May-Hegglin anomaly | Treated with 1 g/day of intravenous methylprednisolone for 3 days, followed by 1 mg/kg/day of oral prednisone with subsequent dose tapering |
References
- Sobel R, Aakalu V, Wladis E. A comparison of endonasal dacryocystorhinostomy and external dacryocystorhinostomy: a report by the American Academy of Ophthalmology. Ophthalmology. 2019;126:1580-1585. doi:https://doi.org/10.1016/j.ophtha.2019.06.009
- Van Swol J, Myers W, Nguyen S. Revision dacryocystorhinostomy: systematic review and meta-analysis. Orbit. 2023;42:1-10. doi:https://doi.org/10.1080/01676830.2022.2109178
- Orsolini M, Schellini S, Souza Meneguim R. Success of endoscopic dacryocystorhinostomy with or without stents: systematic review and meta-analysis. Orbit. 2020;39:258-265. doi:https://doi.org/10.1080/01676830.2019.1677726
- Vinciguerra A, Nonis A, Resti A. Influence of surgical techniques on endoscopic dacryocystorhinostomy: a systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2021;165:14-22. doi:https://doi.org/10.1177/0194599820972677
- Moher D, Liberati A, Tetzlaff J. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6. doi:https://doi.org/10.1371/journal.pmed.1000097
- Haddaway N, Page M, Pritchard C. PRISMA2020: an R package and Shiny app for producing PRISMA 2020 – compliant flow diagrams, with interactivity for optimised digital transparency and open synthesis. Campbell Syst Rev. 2022;18. doi:https://doi.org/10.1002/cl2.1230
- Saini A, Citardi M, Yao W. Office-based sinus surgery. Otolaryngol Clin North Am. 2019;52:473-483. doi:https://doi.org/10.1016/j.otc.2019.02.003
- McElnea E, Smyth A, Dutton A. Assisted local anaesthesia for endoscopic dacryocystorhinostomy. Clin Exp Ophthalmol. 2020;48:841-842. doi:https://doi.org/10.1111/ceo.13762
- Hamal D, Kafle P, Lamichhane B. Endoscopic endonasal dacryocystorhinostomy under local anesthesia or assisted local anesthesia. Nepal J Ophthalmol. 2022;14:10-18. doi:https://doi.org/10.3126/nepjoph.v14i1.21971
- Zhao L, Sun Z, Shen W. Clinical application of dexmedetomidine combined with dezocine in local anesthesia for endoscopic dacryocystorhinostomy. Ear Nose Throat J. Published online 2022. doi:https://doi.org/10.1177/01455613221108366
- Zhang M, Wang X. Rupture of a previously undiagnosed intracranial aneurysm during endoscopic dacryocystorhinostomy: a case report. Clin Case Rep. 2023;16(11). doi:https://doi.org/10.1002/ccr3.6749
- Vinciguerra A, Nonis A, Giordano Resti A. Role of anaesthesia in endoscopic and external dacryocystorhinostomy: a meta-analysis of 3282 cases. Eur J Ophthalmol. 2022;32:66-74. doi:https://doi.org/10.1177/11206721211035616
- Lilja M, Leivo T, Uusitalo M. Acute versus late endoscopic dacryocystorhinostomy in treatment of acute dacryocystitis: a prospective randomised trial with an 18-month follow-up. Acta Ophthalmologica. 2024;102:441-447. doi:https://doi.org/10.1111/aos.15752
- Pakdel F, Soleimani M, Kasaei A. Shifting to very early endoscopic DCR in acute suppurative dacryocystitis. Eye. 2020;34:1648-1653. doi:https://doi.org/10.1038/s41433-019-0734-2
- Yu B, Tu Y, Zhou G. Management of chronic dacryocystitis cases after failed external dacryocystorhinostomy using endoscopic technique with a novel lacrimal ostium stent. Int J Ophthalmol. 2022;15:413-419. doi:https://doi.org/10.18240/ijo.2022.03.07
- Sung J, Kim J, Hwang J. Optimal timing for primary early endoscopic dacryocystorhinostomy in acute dacryocystitis. J Clin Med. 2021;10. doi:https://doi.org/10.3390/jcm10102161
- Herzallah I, Marglani O, Alherabi A. Bilateral simultaneous endoscopic dacryocystorhinostomy: outcome and impact on the quality of life of the patients. Int Arch Otorhinolaryngol. 2019;23:191-195. doi:https://doi.org/10.1055/s-0038-1675394
- Matoušek P, Lubojacký J, Masárová M. Does bicanalicular intubation improve the outcome of endoscopic dacryocystorhinostomy?. J Clin Med. 2022;11. doi:https://doi.org/10.3390/jcm11185387
- Yu B, Xia Y, Sun J. Surgical outcomes in acute dacryocystitis patients undergoing endonasal endoscopic dacryocystorhinostomy with or without silicone tube intubation. Int J Ophthalmol. 2021;14:844-848. doi:https://doi.org/10.18240/ijo.2021.06.08
- Yim M, Wormald P, Doucet M. Adjunctive techniques to dacryocystorhinostomy: an evidence-based review with recommendations. Int Forum Allergy Rhinol. 2021;11:885-893. doi:https://doi.org/10.1002/alr.22699
- Li J, Wang J, Sun C. Efficacy of hyaluronic acid in endoscopic dacryocystorhinostomy: a systematic review and meta-analysis. Am J Rhinol Allergy. 2023;37:102-109. doi:https://doi.org/10.1177/19458924221126356
- Chen I, Ayalon H, Drabkin E. Introduction of steroid absorbed spongostan in endoscopic dacryocystorhinostomy improves success rates. Ophthalmic Plast Reconstr Surg. 2022;38:444-447. doi:https://doi.org/10.1097/IOP.0000000000002156
- Kang T, Won Y, Kim J. Efficacy of triamcinolone-soaked nasal packing on endoscopic dacryocystorhinostomy. Ophthalmic Plast Reconstr Surg. 2021;37:S44-S47. doi:https://doi.org/10.1097/IOP.0000000000001791
- Demir D. Is nasal packing necessary after endoscopic dacryocystorhinostomy without stent and mucosal flaps preservation?. J Craniofac Surg. 2021;32:2107-2109. doi:https://doi.org/10.1097/SCS.0000000000007386
- Homer N, Watson A, Nakra T. Post-operative endonasal debridement may improve outcomes of endoscopic dacryocystorhinostomy. Ear Nose Throat J. Published online 2023. doi:https://doi.org/10.1177/01455613231195144
- Kaptı H, Korkmaz H. Evaluation of the efficacy of postoperative triamcinolone in endoscopic dacryocystorhinostomy using lacrimal symptom questionnaire. Int Ophthalmol. 2022;42:2573-2580. doi:https://doi.org/10.1007/s10792-022-02305-6
- Boal N, Chiou C, Sadlak N. Antibiotic utilization in endoscopic dacryocystorhinostomy: a multi-institutional study and review of the literature. Orbit. 2024;43:183-189. doi:https://doi.org/10.1080/01676830.2023.2227705
- Wladis E, Khan H, Chen V. Are systemic antibiotics required during and after dacryocystitis-related dacryocystorhinostomy?. Orbit. 2020;39:413-414. doi:https://doi.org/10.1080/01676830.2019.1704798
- Vinciguerra A, Nonis A, Resti A. Impact of post-surgical therapies on endoscopic and external dacryocystorhinostomy: systematic review and meta-analysis. Am J Rhinol Allergy. 2020;34:846-856. doi:https://doi.org/10.1177/1945892420945218
- Yang J, Cao Z, Gu Z. Modified endoscopic dacryocystorhinostomy using the middle uncinate process approach. J Craniofac Surg. 2020;31:1464-1466. doi:https://doi.org/10.1097/SCS.0000000000006493
- Alicandri-Ciufelli M, Russo P, Aggazzotti Cavazza E. Endoscopic “retrograde” dacryocystorhinostomy: a fast route to the lacrimal sac. Eur Ann Otorhinolaryngol Head Neck Dis. 2023;140:85-88. doi:https://doi.org/10.1016/j.anorl.2022.08.004
- Chang K, Shen Y. Endonasal endoscopic nasolacrimal duct dissection for primary nasolacrimal duct obstruction. Taiwan J Ophthalmol. 2019;10:116-120. doi:https://doi.org/10.4103/tjo.tjo_111_18
- Ciğer E, İşlek A. Lacrimal sac anterior border-maxillary line distance: effect on endoscopic dacryocystorhinostomy (EDCR) surgery results and NLDO-SS questionnaire. Indian J Otolaryngol Head Neck Surg. 2022;74:1382-1387. doi:https://doi.org/10.1007/s12070-021-02524-w
- Wang Y, Liu F, Cao M. Efficacy and safety of modified seamless endoscopic dacryocystorhinostomy in patients with chronic dacryocystitis. J Ophthalmol. Published online 2022. doi:https://doi.org/10.1155/2022/3061859
- Chen R, Liu S, Jiang A. A simple and efficient technique for suturing and knotting during endoscopic dacryocystorhinostomy. Int Ophthalmol. 2023;43:63-71. doi:https://doi.org/10.1007/s10792-022-02388-1
- Wang D, Fang P, Zhao Y. Assessment of long-term outcomes associated with a lobulated pedicled nasal mucosa flap technique for endoscopic dacryocystorhinostomy without stenting. Ear Nose Throat J. 2021;100:618S-623S. doi:https://doi.org/10.1177/0145561319900025
- Bani-Ata M, Aleshawi A, Ahmad M. Endoscopic dacryocystorhinostomy: a comparison of double-flap and single-flap techniques. Ann Med Surg. 2020;54:1-5. doi:https://doi.org/10.1016/j.amsu.2020.03.005
- Cong T, Wu Y, Gao Y. Modified endoscopic dacryocystorhinostomy: a clubhead-shaped nasal mucoperiosteal flap technique. Laryngoscope. 2022;132:2314-2318. doi:https://doi.org/10.1002/lary.30265
- Ceylan S, Erdoğan C, Sozen T. The fibrin glue application enhances surgical success rate in endonasal endoscopic dacryocystorhinostomy with lacrimal sac preservation. Ear Nose Throat J. 2021;100:483S-488S. doi:https://doi.org/10.1177/0145561319882123
- Zloto O, Koval T, Yakirevich A. Endoscopic dacryocystorhinostomy with and without mucosal flap-is there any difference?. Eye. 2020;34:1449-1453. doi:https://doi.org/10.1038/s41433-019-0716-4
- Kingdom T, Barham H, Durairaj V. Long-term outcomes after endoscopic dacryocystorhinostomy without mucosal flap preservation. Laryngoscope. 2020;130:12-17. doi:https://doi.org/10.1002/lary.27989
- Ciğer E, İşlek A. Mucosal healing with lacrimal and double mucosal flaps endoscopic dacryocystorhinostomy – comparison with flap sacrificed technique: randomised, controlled study. J Laryngol Otol. 2022;136:1189-1195. doi:https://doi.org/10.1017/S0022215121004059
- Vatansever M, Dursun Ö. Endoscopic dacryocystorhinostomy with modified mucosal flap technique. J Craniofac Surg. 2023;34:E216-E218. doi:https://doi.org/10.1097/SCS.0000000000009054
- Woo M, Yang S, Park J. Surgical outcomes of endoscopic conjunctivodacryocystorhinostomy using a castroviejo double-ended lacrimal dilator. J Craniofac Surg. 2020;31:1449-1451. doi:https://doi.org/10.1097/SCS.0000000000006412
- Ushio M, Masahara H, Sakamoto M. Conjunctivoductivo-dacryocystorhinostomy: a novel surgery for intractable canalicular obstruction. Laryngoscope. 2022;132:728-731. doi:https://doi.org/10.1002/lary.29861
- Koval T, Zloto O, Yakirevitch A. No impact of nasal septoplasty on the outcome of endoscopic dacryocystorhinostomy. Eye. 2020;34:1454-1458. doi:https://doi.org/10.1038/s41433-019-0696-4
- Tachino H, Takakura H, Shojaku H. Flap suturing endonasal dacryocystorhinostomy assisted by ultrasonic bone aspirator. Acta Otolaryngol. 2022;142:316-322. doi:https://doi.org/10.1080/00016489.2022.2041721
- Boehm F, Friedrich D, Sommer F. Nasolacrimal duct stenosis-Surgery with a novel robotic endoscope positioning system. Int J Med Robot. 2020;16:1-5. doi:https://doi.org/10.1002/rcs.2144
- Mihailovic N, Blumberg A, Rosenberger F. Long-term outcome of transcanalicular microdrill dacryoplasty: a minimally invasive alternative for dacryocystorhinostomy. Br J Ophthalmol. 2021;105:1480-1484. doi:https://doi.org/10.1136/bjophthalmol-2020-316146
- Poignet B, Sultanik P, Beaujeux P. Primary balloon dacryoplasty for nasolacrimal duct obstruction in adults: a systematic review. Orbit. 2021;40:455-460. doi:https://doi.org/10.1080/01676830.2020.1818264
- Winebrake J, Mahrous A, Kacker A. Postoperative bioresorbable chitosan-based dressing for endoscopic middle meatal dacryocystorhinostomy with balloon dilation. Ear Nose Throat J. 2021;100:425-429. doi:https://doi.org/10.1177/0145561319866822
- Kumar S, Mishra A, Sethi A. Comparing outcomes of the standard technique of endoscopic DCR with its modifications: a retrospective analysis. Otolaryngol Head Neck Surg. 2019;160:347-354. doi:https://doi.org/10.1177/0194599818813123
- Keren S, Abergel A, Manor A. Endoscopic dacryocystorhinostomy: reasons for failure. Eye. 2020;34:948-953. doi:https://doi.org/10.1038/s41433-019-0612-y
- García Callejo F, Juantegui Azpilicueta M, Balaguer García R. Factors involved in the success and failure of endoscopic dacryocystorhinostomy from our experience. Acta Otorrinolaringol Esp. 2022;73:11-18. doi:https://doi.org/10.1016/j.otoeng.2020.09.005
- Cohen O, Amos I, Halperin D. Five- and 10-year outcomes for primary endoscopic dacryocystorhinostomy: failure rate and risk factors. Laryngoscope. 2021;131:10-16. doi:https://doi.org/10.1002/lary.28528
- Wang Y, Jiang W, Tu Y. Endoscopic dacryocystorhinostomy with mucosal anastomosing in chronic dacryocystitis with three categories of ethmoid sinuses. Int J Ophthalmol. 2022;15:1765-1771. doi:https://doi.org/10.18240/ijo.2022.11.06
- Allon R, Cohen O, Bavnik Y. Long-term outcomes for revision endoscopic dacryocystorhinostomy-the effect of the primary approach. Laryngoscope. 2021;131:E682-E688. doi:https://doi.org/10.1002/lary.28795
- Kim S, Kim C, Park J. Salvage of impending rhinostomy failure after dacryocystorhinostomy with office-based microdebrider treatment. Graefes Arch Clin Exp Ophthalmol. 2022;260:1315-1321. doi:https://doi.org/10.1007/s00417-021-05421-8
- Vinciguerra A, Indelicato P, Giordano Resti A. Long-term results of a balloon-assisted endoscopic approach in failed dacryocystorhinostomies. Eur Arch Otorhinolaryngol. 2022;279:1929-1935. doi:https://doi.org/10.1007/s00405-021-06975-3
- Mueller S, Freitag S, Lefebvre D. Revision eDCR using a superior pedicled mucosal flap. Orbit. 2019;38:1-6. doi:https://doi.org/10.1080/01676830.2018.1444062
- Hsu C, Lee L, Kuo B. Surgical and anatomic consideration in endoscopic dacryocystorhinostomy of a patient with damaged sinonasal anatomy post-Caldwell-Luc surgery: a case report. Medicina. 2022;58. doi:https://doi.org/10.3390/medicina58010078
- Gupta N, Ganesh S, Singla P. A rare association of blepharophimosis-ptosis-epicanthus inversus case with congenital nasolacrimal duct obstruction. Eur J Ophthalmol. 2021;31:NP8-NP11. doi:https://doi.org/10.1177/1120672119886427
- Sagar P, Shankar R, Wadhwa V. Primary tubercular dacryocystitis – a case report and review of 18 cases from the literature. Orbit. 2019;38:331-334. doi:https://doi.org/10.1080/01676830.2018.1513044
- Song X, Yang J, Lai Y. Localized amyloidosis affecting the lacrimal sac managed by endoscopic surgery: a case report. World J Clin Cases. 2020;8:5684-5689. doi:https://doi.org/10.12998/wjcc.v8.i22.5684
- Nassif S, Ruiz D, Callahan A. Nasolacrimal duct obstruction: an unusual presentation of sarcoidosis. Ear Nose Throat J. 2022;101:NP143-NP145. doi:https://doi.org/10.1177/0145561320950494
- Azhdam A, Wang Y, Douglas R. Angioleiomyoma of the nasolacrimal duct: case report and literature review. Orbit. 2022;41:783-785. doi:https://doi.org/10.1080/01676830.2021.1933080
- Lee J, Lee D. Delayed unilateral pneumocephalus after bilateral endoscopic dacryocystorhinostomy in an elderly patient. BMJ Case Rep. 2021;14. doi:https://doi.org/10.1136/bcr-2020-241540
- Galindo-Ferreiro A, Torres Nieto M, Ali M. Orbital fat necrosis following a revision endoscopic dacryocystorhinostomy. Eur J Ophthalmol. 2021;31:NP18-NP21. doi:https://doi.org/10.1177/1120672120932087
- Cheong T, Davies R. Meningoencephalitis following endoscopic dacryocystorhinostomy. Ophthalmic Plast Reconstr Surg. 2019;35:E47-E49. doi:https://doi.org/10.1097/IOP.0000000000001324
- Gungel H, Altan C, Karini B. Contralateral vision loss after endonasal dacryocystorhinostomy: a case report of purtscher-like retinopathy and treatment with intravitreal tissue plasminogen activator. Retin Cases Brief Rep. 2019;13:255-259. doi:https://doi.org/10.1097/ICB.0000000000000574
- Bladen J, Siah W, Tan P. Peri-orbital surgical emphysema following endoscopic dacryocystorhinostomy. J Laryngol Otol. Published online 2020:1-3. doi:https://doi.org/10.1017/S0022215120001875
- Bothra N, Bejjanki K, Ali M. Gossypibioma: an unusual complication of an endoscopic dacryocystorhinostomy. Indian J Ophthalmol. 2020;68:2247-2248. doi:https://doi.org/10.4103/ijo.IJO_2225_19
- Lee S, Huh H, Cho H. A case report of optic neuropathy following dacryocystorhinostomy in a 57-year-old female patient with May-Hegglin anomaly. BMC Ophthalmol. 2020;20. doi:https://doi.org/10.1186/s12886-020-01433-w
Downloads
 PDF
PDF
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2024 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 601 times
- PDF downloaded - 203 times